Alterations of the default mode network connectivity in obsessive-compulsive personality disorder
A Pilot Study
Originally published by: ScienceDirect
Written by: Joana Coutinho, PhD, Oscar Filipe Goncalves, José Miguel Soares, Paulo Marques, Adriana Sampaio
Obsessive-compulsive personality (OCPD) disorder is characterized by a pattern of excessive self-control, perfectionism and behavioral and cognitive rigidity. Despite the fact that OCPD is the most common personality disorder in the general population, published studies looking at the brain correlates of this disorder are practically nonexistent. The main goal of this study was to analyze the presence of brain alterations in OCPD when compared to healthy controls, specifically at the level of the Default Mode Network (DMN). The DMN is a well-established resting state network which was found to be associated with psychological processes that may play a key role in OCPD (e.g., self-awareness, episodic future thinking and mental simulation). Ten individuals diagnosed with OCPD and ten healthy controls underwent a clinical assessment interview and a resting-state functional magnetic resonance imaging (fMRI) acquisition. The results show that OCPD patients presented an increased functional connectivity in the precuneus (i.e., a posterior node of the DMN), known to be involved in the retrieval manipulation of past events in order to solve current problems and develop plans for the future. These results suggest that this key node of the DMN may play an important role in the pathophysiology of OCPD.
1. Introduction
Obsessive-compulsive personality disorder (OCPD) was one of the first identified personality disorders (American Psychiatric Association, 1952). A central dimension of this disorder is the need for control: control over the self and over the environment. This need of control is associated with clinical symptoms such as excessive concern with lists, rules and minor details, perfectionism, excessive devotion to work, moral rigidity, inability to discard worthless objects and to delegate responsibilities to others, rigidity and stubbornness (American Psychiatric Association, 2000). These clinical symptoms may result in a significant impairment in social, work and/or family functioning (Mancebo et al., 2005; Skodol et al., 2002), due to these patients' rigidity and consequent difficulties in establishing and maintaining close relationships (American Psychiatric Association, 2013). These symptoms also interfere with subjective well-being due to OCPD patient's difficulties in relaxing, and dealing with the unpredictability of daily life and an internal speech marked by self-blame, perfectionist and ruminative thinking (Pinto et al., 2014).
The prevalence of OCPD in outpatient settings is between 8% and 9% (Cain et al., 2014). Despite the fact that OCPD, unlike other personality disorders, has been included in all the revisions of the DSM, including its fifth edition, and the fact that it is the most common personality disorder in the general population (de Reus and Emmelkamp, 2012; Grant et al., 2012), very little is known about its neural basis.
In fact, contrarily to Obsessive Compulsive Axis I disorder in which abundant neuroimaging research is available (e.g., Stern et al., 2012; Fitzgerald et al., 2010; Peng et al., 2014), there are, to the best of our knowledge, no functional neuroimaging studies in OCPD. The absence of empirical findings on the neural correlates of OCPD may be related with the difficulties in recruiting these patients for MRI studies. Indeed some of the clinical features of this disorder make these patients quite reluctant in doing an MRI acquisition due to the uncontrollability (e.g., possibility of discovering some health problem in the brain, claustrophobia and noise created by the scanner) inherent to the procedure.
The aim of this study is precisely to fill this gap in the literature, by analyzing the brain correlates of OCPD focusing on a specific neural network: The Default Mode Network (DMN). The DMN is a network of several brain regions that show high levels of metabolic activity when no explicit task is performed and the subjects are asked simply to rest (Raichle et al., 2001). The brain regions that compose the DMN include the posterior cingulate cortex (PCC) and adjacent precuneus, the medial prefrontal cortex (mPFC) and the bilateral inferior parietal cortex and medial temporal cortex (Buckner et al., 2008; Fox and Raichle, 2007; Raichle et al., 2001). There are other known resting state networks that represent the spontaneous neuronal activity intrinsically generated by the brain under resting conditions, but a specificity of the DMN is the fact that it demonstrates a pattern of deactivation during the initiation of task-related activity focused on external stimuli such as working memory or cognitive control tasks (Buckner et al., 2008; Raichle and Snyder, 2007).
There is evidence that the DMN plays a role in several psychological processes that may be relevant in the pathophysiology of OCPD, namely: introspective and reflective self-awareness processes (Buckner et al., 2008), thinking about one's future (Schacter et al., 2007), mental simulation and planning (Hassabis and Maguire, 2007), perspective-taking (Buckner and Carroll, 2007) and mind wandering (Andrews-Hanna, 2012; Christoff et al., 2009). In fact, in a study by Delamillieure et al. (2010), the authors did an introspective evaluation of the inner experience of participants undergoing fMRI in the resting state. For that 180 participants completed the ReSQ – Resting State Questionnaire (in which they rate the proportion of time spent in each mental activity during the resting state fMRI) immediately after being scanned with fMRI while at rest. They found that the majority of participants reported either retrospective memories (82%) or prospective thoughts (78%), related to the future.
Some of these mental processes previously associated with the activity of the DMN, have been found to be altered in OCPD, namely patients' propensity for self-referent thoughts, to rethink about the recent past and to imagine future events in an attempt to increase control and decrease uncertainty (Pinto et al., 2014). Thus, we may hypothesize that, in a resting state fMRI acquisition in which patients are left to their own thoughts (i.e., not involved in any specific cognitive task), OCPD patients may be more likely to get involved in the type of cognitive processes associated with the DMN (e.g. thinking about concerning events or planning the future) due to their rumination or perfectionism. If this is the case, an increased functional connectivity in the DMN may be expected in OCPD individuals when compared with healthy controls.
Even though no published fMRI resting state studies have been conducted in OCPD, several disorders that frequently co-occur with OCPD (e.g, generalized anxiety disorder, depression and even obsessive compulsive (OCD) Axis I disorder) were found to present impaired DMN activation patterns. For example, in depression it was found an increase in DMN resting-state functional connectivity (e. g., Zhou et al., 2010; Hamilton et al., 2011). Importantly, DMN alterations in depression were found to be associated with higher levels of maladaptive rumination (Grimm et al., 2009; Kross et al., 2009). In fact rumination, which is also prevalent in OCPD, has been associated with altered activation in the DMN, including in the mPFC and the PCC (Christoff et al., 2009; Mason et al., 2007; Stawarczyk et al., 2011).
Studies conducted with OCD patients have also showed evidence for an increased connectivity in several areas of default mode network including PCC/precuneus (Stern et al., 2012). Also the medial frontal cortex presented alterations in functional connectivity in OCD (Fitzgerald et al., 2010). However there are also reports of a decreased DMN connectivity in OCD patients (Peng et al., 2014).
Finally, evidence from personality neuroscience which studies the neurobiological basis of different personality traits, has shown that normal variation in traits associated with OCPD such as conscientiousness (Douglas and Thomas, 2011) – the Big Five personality trait involving perfectionism, inhibition, self-discipline and planning - is related with DMN alterations. Specifically, previous studies have shown that higher levels of Conscientiousness were associated with structural alterations (e.g., DeYoung et al., 2010) as well as with increased activation of the DMN bilateral parietal cortex (e.g., Sampaio et al., 2013).
Given that the DMN is associated with psychological processes found to be impaired in OCPD and based on indirect evidence from alterations of the DMN found in other disorders that share common psychological features, we hypothesize that OCPD individuals will present an increased functional connectivity of the DMN, both in the posterior DMN regions such as PCC/precuneus involved in self-referential thoughts focused on future events and planning of activities (e.g. Olson et al., 2007), and in the anterior regions such as the mPFC involved in self-referent thinking (e.g. Gusnard and Raichle, 2001).
It is important to note that although both the anterior and posterior DMN nodes are involved in self-referential thought, there is a growing consensus that there is a functional specialization in these areas in terms of the content of that self-referential activity (e.g., Andrews-Hanna et al., 2010). Whereas frontal regions, such as the mPFC have been linked with emotional self- referent thoughts and self-referential judgments about one's present situation or mental state, posterior regions such as the PCC have been associated with performing episodic judgments about one's personal future, in other words with prospective memory and mental scene construction (e.g., Hassabis and Maguire, 2007; Schacter and Addis, 2007). Therefore these areas may not be equally altered in OCPD patients, being that the PCC node should the one presenting more pronounced differences in functional connectivity when we compare OCPD with controls. This hypothesis is based on these patient ́s focus on controlling the environment and planning the future in detail, which is linked with the prospective thinking and life simulation associated with DMN posterior nodes.
2. Method
2.1 Participants
Twenty-six individuals participated in this study. The experimental group included fourteen participants who filled the diagnostic criteria for obsessive-compulsive personality disorder, matched with healthy controls. However, due to technical problems with the acquisition, three individuals in the OCPD group had to be excluded. One OCPD patient had also to be excluded due to pregnancy. Thus the final experimental group included ten OCPD patients matched by age and gender with ten healthy individuals of the control group. General exclusion criteria for the study were as follows: 1) the presence of any major medical disorder; 2) dependency or abuse in the past year of alcohol and/or drugs; 3) general MRI contraindications (e.g., metallic implants; pregnancy). Participants with co-morbid Obsessive Compulsive Axis I disorder, as well as participants with psychotic symptoms, with substance abuse disorders, depression or anxiety disorders and with other Axis II disorders rather than OCPD (e.g. borderline, paranoid, avoidant or histrionic) were also excluded from the study. Patients were not on psychotropic medication. Participants responded to a laterality test, the Edinburgh Handedness Inventory (Oldfield, 1971) – to ensure that all were right-handed (EHI ≥ 80).

Table 1 - Demographic characteristics for obsessive compulsive personality disorder patients (OCPD) and healthy controls (HC).
Note. The NEO FFI scores presented in this Table have descriptive purposes of the overall personality traits of OCPD and healthy participants. Independent sample t- tests showed no differences between groups in age, years of education or laterality. Group differences in NEO-FI scores were also non-significant.
Participants had a mean age of 38.62 (SD = 8.97), ranging from 23 to 52 years old. Groups did not differ in age [t (18) = 1.02, p = 0.90] or years of education [t (18) = -1.05, p = 0.30] at the time of the scan. Demographic and clinical information of the sample can be found in Table 1.
The study was approved by the University Institutional Review Board of the University. All the procedures complied with the principles expressed in the Declaration of Helsinki. OCPD individuals were recruited in the counseling services of University of Minho and private clinics. The control group was recruited through informal advertisement of the study. For that we looked in the community for healthy individuals with the same age, gender and educational level than OCPD, who volunteered to do a resting fMRI scan. All the participants were informed about the procedures of the study and all gave informed written consent. The participants underwent a session of clinical assessment carried out by a clinical psychologist, to confirm the presence of the OCPD diagnostic criteria and, those included, underwent an fMRI acquisition.
2.2 Clinical assessment
2.2.1 Semi-structured clinical interview for disorders of the DSM - IV - II (SCID II) – (Spitzer, Williams, Gibbon, 1997)
The SCID-II is a version of the SCID developed for the assessment of DSM-IV-TR Personality Disorders. It is a semi-structured interview used to evaluate the ten diagnoses of the Axis II of the DSM-IV. The SCID-II is unique in that it was designed with the primary goal of providing a rapid clinical assessment of personality disorders without sacrificing reliability or validity. It can be used in conjunction with a self-report personality questionnaire, which allows the interview to focus only on the items corresponding to positively endorsed questions on the questionnaire, thus shortening the administration time of the interview. In this study this SCID-II was used to confirm OCPD diagnostic criteria.
2.2.2 NEO – Five Factor Inventory (NEO FFI) – (Costa and McCrae, 1989)
NEO FFI is a self-report personality measure. It is the short version of the NEO PI-R developed with the aim of assessing the five personality domains of the Five-Factor model: Neuroticism (N), Extraversion (E); Openness to Experience (O); Agreeableness (A) and Conscientiousness (C). It provides a global evaluation of the normal adult's personality in different contexts and consists of 60 items used to derive the five personality domain scores (12 items per domain). Each of the five domains of the NEO FFI has been found to have adequate internal consistency: ∝ = .68 to 0.86 (Costa and McCrae, 1992) and temporal stability: r = .86 to 0.90 (Robins et al., 2001). In the Portuguese version (Magalhães et al., 2014) a coherent factor structure with the five-factor model was obtained, explaining 21% of variance, a value similar to the American Version explaining 23% of the variance (Costa et al., 1991). Values of internal consistency (Cronbach Alpha) for the 5 factors ranged between 0.80 for Extraversion and 0.86 for Conscientiousness (Lima, 1997). In this study the NEO FFI was only used as a descriptive measure, thus its results are presented in Table 1 with the purpose of characterizing our sample in terms of the Big 5 personality traits.
2.3 Functional MRI acquisition
Neuroimaging acquisition was performed in a clinically approved Philips Achieva 3 T scanner equipped with an eight-channel head coil, in Centro Hospitalar do Porto. A six minutes resting state functional acquisition was obtained axially using a gradient echo-planar imaging (EPI), BOLD fMRI sequence with 100 volumes and the following imaging parameters: repetition time=3 s, echo time=40 ms, flip angle=90°, field of view=235 mm, slice thickness=3.2 mm, 50 axial slices with a matrix=72 x 74; pixel size=2.9 x 2.9 mm². Participants were instructed to keep their eyes closed and to remain awake but relaxed, doing nothing in particular during the acquisition.
2.4 Image pre-processing
The preprocessing of the fMRI data was performed using BrainCAT (Brain Connectivity Analysis Tool) (Marques et al., 2013). The first step performed by BrainCAT consisted in removing the five initial volumes of the acquisition so that the instability of the main magnetic field at the beginning of the acquisition would not interfere with the results. The removal of the initial volumes was followed by motion correction to compensate for involuntary head movement, so that each anatomical landmark stayed in the same position across all the volumes of the acquisition. BrainCAT corrected this motion with a rigid alignment of all the volumes to the mean of the functional acquisition with a six-parameter rigid-body spatial transformation. Images were spatially normalized to the MNI (Montreal Neurological Institute) standard coordinate system using the default EPI templates in the toolbox and resampled to 2 x 2 x 2 mm³. In order to increase signal-to-noise ratio (SNR) and reduce residual inter-subject miss-registrations, spatial smoothing was applied to the functional volumes, with a Gaussian kernel of 8 x 8 x 8 mm. This was done by the convolution of the images with a tridimensional Gaussian function, with the resulting voxels representing a weighted mean of itself and the neighboring voxels. For that we specified the full width at half maximum (FWHM) to 8 mm to control the extent of smoothing. Finally, a band-pass filter with a default value (0.01–0.08 Hz) was applied to the time series of each voxel to reduce the effects of low-frequency drift and high-frequency noise.
2.5 Independent component analysis
After preprocessing the data, we started the fMRI analysis in BrainCAT by performing an Independent Component Analysis (ICA) of the fMRI data. For that we used the concatenation approach for decomposition of MELODIC in order to search for common spatial patterns among subjects and allowed MELODIC to automatically estimate the number of independent components to extract. The components estimated for each subject represent the independent sources of variability in the resting state data. After the component estimation we used a dual_regression in order to retrieve each subject's version of the group components. This enabled us to further use these estimates to perform group comparisons. After performing group ICA, we selected the component of interest (the one that corresponded to the DMN) based on visual inspection. For this purpose, BrainCAT called fslview, a viewer distributed with FSL, and loaded the 4D dataset containing all the estimated components overlaid on the MNI 152 T1 template. Finally, a study-specific mask of the DMN was generated by thresholding the corresponding Z-score group map to Z43.09 (po0.001) and then binarizing this thresholded map.
2.6 Statistical analyses
The DMN component of each subject (z-maps) was used to perform group statistical analyses. The Statistical analyses using the second level random effect was performed on SPM12 (Statistical Parametrical Mapping) in two steps. First, we performed a one sample t-test to confirm the DMN activation in both groups and study the global pattern of DMN activation at the group level. For this all the individual default mode z maps that were extracted in the ICA analyses were included. The same DMN template mask that has been used to sort the components of the ICA was applied to extract results.
Then a directional two sample t-test was used for between groups comparison. All the results were corrected for multiple comparisons using a cluster-based correction. First the smoothness of the residuals of the statistical model was estimated using the “3dFWHMx” program distributed with AFNI (http://afni.nimh. nih.gov), resulting in an estimated smoothness of 8.21593 mm x 10.8715 mm x 11.5338 mm within the mask. Afterwards, the minimum cluster size necessary to achieve a threshold of p < 0.05 fully corrected for multiple comparisons was computed with “3dClustSim” also distributed with AFNI. Using a cluster-defining threshold of p < 0.01 and the smoothness estimate of the residuals, this resulted in a minimum cluster size of 156 voxels.
3. Results
3.1 DMN global activation pattern
The DMN was identified in the resting state condition for the entire sample (N=20). As can be seen in Fig. 1, the main DMN anatomical areas, namely the PCC and precuneus, the mPFC, the bilateral inferior parietal cortex and the left inferior temporal cortex, were identified.

Fig. 1. DMN activation identified in the resting state condition for the entire sample (p < 0.05 FWE corrected). A sagittal section showing the medial prefrontal cortex and the posterior cingulate cortex (left image); a coronal section showing the posterior cingulate cortex and parietal cortex (middle image) and an axial section (right image) showing the medial prefrontal cortex, posterior cingulate cortex and lateral parietal cortex.
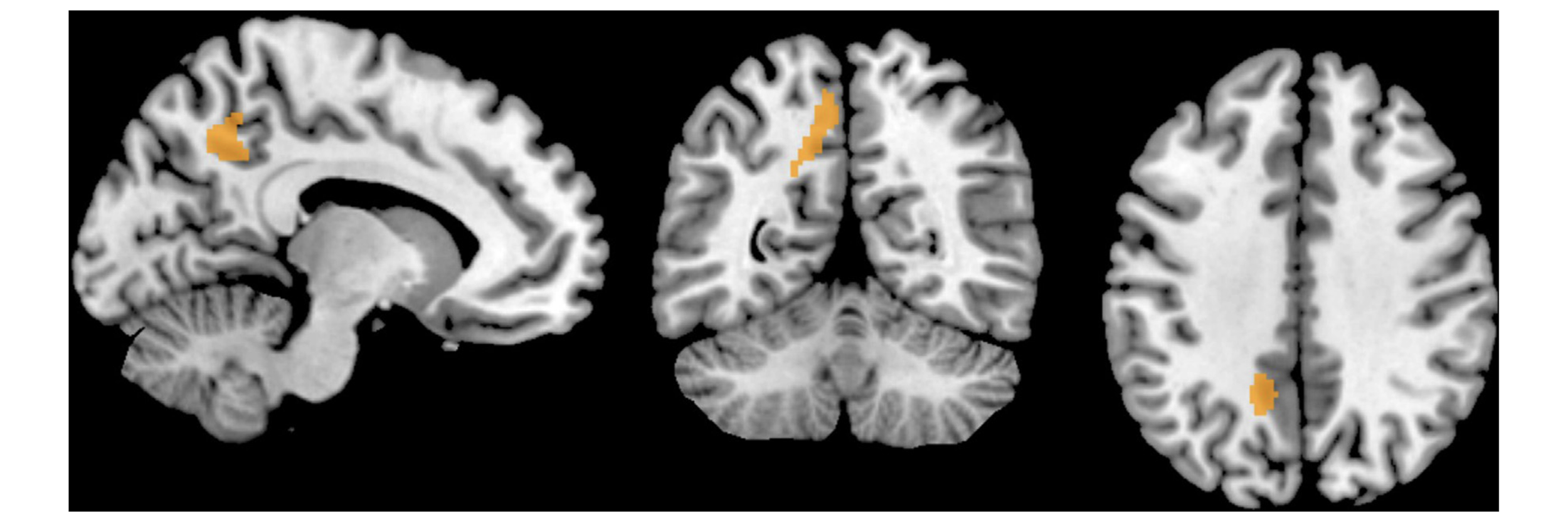
Fig. 2. Left Precuneus showing an increased functional connectivity in OCPD patients seen on sagittal (left), axial (in the middle) and coronal (right) views.
3.2 DMN differences between OCPD and Controls
Individuals with OCPD presented increased levels of functional connectivity in the left precuneus (MNI coordinates: x = -14, y= -52, z=40; Cluster size: 166 voxels; t=4.32, Z=3.56) when compared with heathy controls. The results were significant at a corrected for multiple comparisons p < 0.05 threshold determined by Monte Carlo simulation program (AlphaSim) (Fig. 2).
4. Discussion
The present study constituted, to the best of our knowledge, a first attempt to explore the presence of alterations in the DMN functional connectivity in a sample of OCPD patients. We found that when compared with healthy controls, OCPD patients presented a higher functional connectivity in one key area of the posterior DMN: the precuneus. No significant differences were found in anterior nodes of the DMN (e.g., mPFC), contrarily to our hypothesis that predicted an increased functional connectivity in both anterior and posterior regions of the DMN.
Previous research showed evidence for a functional specialization of the anterior and posterior regions of the DMN (e.g., Northoff et al., 2006; Zhao et al., 2007; Greicius et al., 2007; Zhu, 2012; Coutinho et al., 2015). The anterior DMN regions, such as the mPFC are tightly connected with limbic areas and as such more involved in the emotional self-referential processing (Ochsner and Gross, 2005; d’d’Argembeau et al., 2005). The posterior regions, such as the PCC and temporal areas, are densely connected with the hippocampus, and seem to be more involved in tasks such as autobiographic episodic memory and performing episodic judgments about the future (Behrmann et al., 2004; DeYoung et al., 2010).
In a previous study Andrews-Hanna and colleagues (2010) analyzed the functional-anatomic fractionation of the DMN, using an fMRI paradigm that allowed prospective, episodic decisions about one's personal future (Future Self) to be compared to self- referential judgments about one's present situation or mental state (Present Self). The authors found that while both conditions activated the midline core, the two DMN subsystems showed selective increases in activation. The medial temporal subsystem was preferentially activated in the future self condition, whereas the medial prefrontal subsystem was preferentially activated during the present self condition. This study was able to clarify the differential contributions of each component of the DMN. Its findings allowed us to overcome the debate between authors that empathize the role of the DMN for prospective memory and mental scene construction (e.g., Hassabis and Maguire, 2007; Schacter and Addis, 2007) and those that emphasize the role of the DMN for self-referential cognition (D’Argembeau et al., 2005) or social processes (Mitchell, 2006; Schilbach et al., 2008), showing that both processes are present but rely in distinct functional-anatomic components within the DMN.
Based on these findings we may assume that different psychological disorders are likely to present different alterations in those distinct DMN components. Thus the functional dissociation among anterior and posterior DMN regions previously reported in the literature (Greicius et al., 2007; Zhu et al., 2012; Coutinho et al., 2015), may offer a possible explanation for our results in which OCPD patients presented an increased functional connectivity only in the posterior nodes of the DMN, particularly in the precuneus, but no differences were found in the anterior nodes such as the MPFC.
The precuneus has been shown to support self-reflection (Johnson et al., 2002; Northoff and Bermphol, 2004), episodic imagery (Fletcher et al., 1996), the retrieval or consolidation of autobiographical memory (Maddock, 1999; Maddock et al., 2001), the conscious representation of information in the form of mental images and spontaneous thoughts, and the manipulation of this information for problem-solving and planning (Cavanna and Trimble, 2006; Vogt and Laureys, 2005; Vogt and Devinsky, 2000). Thus, the posterior nodes of the DMN seem to act as a kind of “life simulator”, in which individuals get involved in when left to think to themselves undisturbed. In fact, during a conscious resting state, individuals report thinking about personally important or concerning events (Singer, 1966; Klinger and Cox, 1987), most of which are future oriented (Andreasen et al., 1995; Andrews-Hanna et al., 2012).
From a psychological perspective, this ability to simulate future events in an effort to solve problems and develop future plans has an important adaptive value because it allows us to adapt our behavior in an attempt to cope with anticipated needs or goals (Addis et al., 2007; Suddendorf and Busby, 2005). However, OCPD patients may get over involved in this anticipatory or prospective process, which leads to symptoms such as rumination on future-oriented planning at the cost of present moment experience and an attentional bias to minor details (Ansell et al., 2010). Our results may suggest the possible role of the posterior DMN nodes on these symptoms.
In order to better understand the role of the DMN in OCPD, future studies should perform a more in-depth clinical assessment of OCPD related symptoms, by administering instruments such as the Perfectionism Inventory (Hill et al., 2004); the Barret Impulsivity Scale (Patton and Stanford, 1995) or the Ruminative Response Scale (Treynor et al., 2003) and analyze the correlations between the scores on these clinical measures and brain resting state connectivity.
Future studies could also assess the content of the patients’ thoughts or feelings during the resting state acquisition, which can be done using measures such as the Resting State Questionnaire (Delamillieure et al., 2010) or the Amsterdam Resting State Questionnaire (Diaz et al., 2013), in which the participant is asked to retrospectively rate the proportion of time spent in different mental activity during the resting-state fMRI acquisition. This would allow us to link resting-state connectivity patterns to specific clinical symptoms and thus extend the clinical significance of our findings. For example, whether OCPD patients who reported more ruminative perfectionist thoughts or concerns with lists and future tasks, were the ones presenting a higher increased in DMN functional connectivity. This is particularly important considering the point made by some authors that fMRI-bold connectivity may reflect a combination of ongoing mental processes and more stable anatomical connectivity. (Barttfled et al., 2015). Indeed the inquire about the participants ́ specific thoughts during the resting acquisition would allow us to ensure the sensitivity of our method to online changes in mental activity.
The small sample size constitutes a limitation of our study. Indeed the personality features of this clinical group made the task of recruiting OCPD patients willing to undergo an fMRI assessment particularly difficult. The MRI involves some degree of uncontrollability, extreme noise as well as some claustrophobia and OCPD patients tended to ruminate about the magnetic resonance imaging procedure, with some individuals refusing to participate. In addition we also lost four patients due to technical problems.
However, despite the modest sample size our results survived the multiple comparisons correction and suggest that the hyperconnectivity of the precuneus – a key node of the DMN - may constitute an important neural marker in the pathophysiology of OCPD. Therefore although preliminary, our findings may have clinical implications for our understanding of OCPD symptoms such as the deficits in cognitive flexibility, experience of unstructured time as intolerable and need to plan out their activities to the minute.
Acknowledgments
This study was conducted at Psychology Research Centre (UID/ PSI/01662/2013), University of Minho, and supported by the Portuguese Foundation for Science and Technology and the Portuguese Ministry of Education and Science through national funds and co-financed by FEDER through COMPETE2020 under the PT2020 Partnership Agreement (POCI-01-0145-FEDER-007653).
Joana Coutinho was funded by a FCT postdoctoral grant (number: SFRH/BPD/75014/2010) and Bial Foundation (grant number 87/12).
J.C., O. G. and A.S. developed the study concept. J.C and A.S. performed the data collection. J. C., M.G. and P. M. performed the data analysis. J.C. drafted the paper and O.G. and A. S. provided critical revisions. All authors approved the final version of the paper for submission.
References available in original article on ScienceDirect.