The role of personality disorders in obsessive-compulsive disorder
Originally published by: Indian Journal of Psychiatry
Additional Authors: Khanna, Sumant
Personality disorders are a common comorbidity in obsessive-compulsive disorder (OCD). The effect of comorbidity on the symptom presentation, course, and treatment outcome of OCD is being discussed here. OCD and obsessive-compulsive personality disorder (OCPD) though similar in their symptom presentation, are distinct constructs. Schizotypal disorder, OCPD, and two or more comorbid personality disorders have been found to be consistently associated with a poor course of illness and treatment response. Further research is needed to determine treatment strategies to handle the personality pathology in OCD.
INTRODUCTION
Comorbid diagnoses in obsessive-compulsive disorder (OCD) are not uncommon. Among all anxiety disorders, the risk of having at least one comorbid personality disorder is the highest for OCD (52%). Hence, it is imperative to understand what impact those comorbidities have on the management and prognosis of OCD.
Personality disorders have been defined as a pervasive maladaptive pattern of behaviors and traits which cause substantial distress and impairment in the socio-occupational functioning of a person. This article attempts to describe the common personality disorders comorbid with OCD and their impact on the course and outcome of OCD.
OBSESSIVE-COMPULSIVE PERSONALITY DISORDER
Among all the personality disorders, obsessive-compulsive personality disorder (OCPD) is perhaps most commonly linked with OCD. It is characterized by a maladaptive pattern of excessive preoccupation with detail and orderliness, excessive perfectionism, and need for control over one's environment. Perfectionism though considered a desirable trait in most cultures, in OCPD it is so excessive that it interferes with task completion. Further, these individuals usually have poor cognitive flexibility and excessive need to control which results in significant dysfunction in socio-occupational domains.
Diagnostic criteria
The Diagnostic and statistical manual of mental disorders-5 (DSM-5) has retained all the eight criteria of the earlier DSM-4 [Table 1]. The older DSM-3 had additional criteria of restricted expression of emotions and indecisiveness which were removed in view of their low specificity. International classification of diseases-10 (ICD-10) is much more liberal in its diagnosis as only 3 out of 8 criteria is enough compared to 4 out of 8 for DSM-5. ICD 10 also does not include miserliness and hoarding in its diagnostic criteria and instead has included excessive doubts and intrusive thoughts. The ICD-10 criteria have an overlap with OCD and anxiety disorders which may lead to conceptual difficulties in distinguishing between them.

Table 1. DSM - 5i and ICD 10 criteria of obsessive-compulsive personality disorder
The ICD-11 beta version description of personality disorders moves away from a categorical model to a dimensional model which evaluates the severity of the disorder and five trait domains, namely, negative affectivity, detachment, disinhibition, dissociality and anankastia. However, a trait domain is coded if its features are prominent in an individual's personality and are causing interference. It also allows multiple trait domains to be coded to specify the personality problems.
Prevalence and course
Even though earlier considered to have lower prevalence, recent community studies have estimated a prevalence of OCPD at 7.2%–7.7%. In the clinical population, the rates are as high as 26%. It is conventionally considered to be more common in males than females, but larger epidemiological studies have not found any gender difference in its prevalence.
There is enough evidence to suggest that the different symptoms of OCPD begin in childhood. In a retrospective study, most individuals dated their symptoms starting in childhood. In fact, a large epidemiological study found that about 13.5% of the youth (n = 733) met the criteria of OCPD.
Studies examining the temporal diagnostic stability of OCPD have yielded conflicting results. In a 2 years longitudinal study, only one-third of patients
Based on similarities with OCD in terms of age of onset, chronicity of illness, symptom similarity, shared heritability, increased comorbidity, shared neurocognitive deficits and treatment response, some researchers advocate the inclusion of OCPD within the obsessive-compulsive and the related disorders (OCRD) section in the upcoming ICD-11. However, the beta version of the ICD-11 and the DSM-5, both do not include OCPD in the OCRD section.
Differentiating obsessive compulsive disorder and obsessive compulsive personality disorder
Even though there are superficial similarities between the two disorders [Table 2], both have been described as separate and distinct conditions.
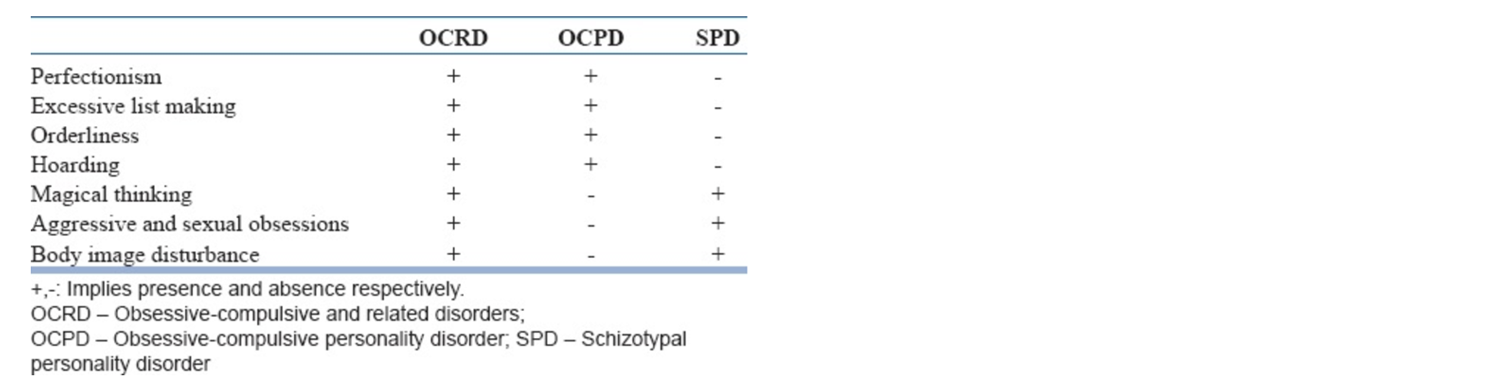
Table 2. Overlap of symptom domains between obsessive-compulsive and related disorders, obsessive-compulsive personality disorder, and schizotypal personality disorder
OCPD and OCD both overlap in terms of stereotyped and inflexible thoughts and behaviors involving orderliness, perfectionism, and list making. However, in OCPD such behaviors are pervasive in all aspects of a person's functioning, whereas in OCD, it is usually restricted to one particular domain. More importantly, in OCPD, such thoughts and behaviors are egosyntonic compared to egodystonic thoughts and behaviors in OCD. Hence, most patients with OCPD tend to present to clinicians with primary complaints of anxiety, depression, or sexual dysfunction rather than core symptoms of personality.
Comorbidity between obsessive-compulsive disorder and obsessive-compulsive personality disorder
OCPD has been found to occur commonly in individuals with OCD with comorbidity rates reported from 15% to 28%. In the light of new hoarding disorder in DSM-5, questions are being raised about how much the previously estimated comorbidity could be explained by the common hoarding symptom between OCD and OCPD. The converse has not been found to be true. In fact, the most common comorbidity found in OCPD was depression.
Nerobiology
Twin studies have a heritability estimate of 0.78 for DSM-3-R OCPD. Increased frequency of OCPD has been found in first-degree relatives of OCD probands compared to relatives of healthy controls.
There are only a handful of studies exploring into the genetic basis of OCPD. One meta-analysis of 3 studies found that individuals with D3 receptor Gly/Gly genotype at the Ser9Gly polymorphism is 2.4 times more likely to have OCPD diagnosis. Another study compared individuals with OCD, panic disorder, OCPD and healthy controls and found no difference in allelic frequencies of the serotonin transporter gene in individuals with OCPD.
Compared to OCD patients and healthy controls, OCPD patients had greater ability to delay reward. They also exhibit a significantly higher capacity to delay reward which is one component of self-control. This is in line with the clinical presentation of OCPD patients who have excessive need to control their environment. Another study found cognitive inflexibility and executive planning deficits when compared to healthy controls in individuals with OCPD.
Treatment
There is a paucity of research into the treatment of OCPD. With respect to pharmacotherapy, there has been only a small (n = 24) randomized placebo-controlled trial using fluvoxamine for 12 weeks. The fluvoxamine group had a significant reduction in personality scores compared to placebo suggesting OCPD traits may also respond to selective serotonin reuptake inhibitor (SSRI) just like in OCD.
There is limited literature on the efficacy of psychotherapy; most of the literature involves case series or uncontrolled trials. Supportive-expressive psychodynamic sessions with OCPD patients were found to show improvement in functioning, anxiety and depressive symptoms posttreatment. Interestingly, cognitive behavior therapy (CBT) has not been well studied so far in OCPD. The largest study with 116 OCPD patients found that baseline anxiety was a significant predictor of response with 10 weekly group CBT. However, this study did not have a control group.
Impact of comorbid obsessive-compulsive personality disorder on obsessive-compulsive disorder
OCD comorbid with OCPD is associated with a younger age of onset, a greater severity, poorer insight, higher comorbid depression or anxiety, and greater impairment in functioning. Most consistent finding in the study of OCD with comorbid OCPD is that such patients were more likely to have “not just right experiences,” hoarding, symmetry, ordering, counting, and arranging symptoms. In the Brown longitudinal obsessive-compulsive study, comorbid OCPD was associated with twice the risk of relapse following remission at 5 years follow up.
Preliminary findings suggest that OCPD may interfere in treatment outcomes of OCD, especially in CBT. There can be a poor motivation to change in OCPD, especially if their obsessions are in line with their personal values. On the other hand, perfectionism can become an asset in treatment as patients will carry out their homework assignments diligently. The evidence also has yielded mixed results. In an open-label trial with exposure and response prevention (ERP), OCPD as a diagnostic category and as a dimensional score predicted a poorer outcome. Within the OCPD criteria, only perfectionism predicted the poorer outcome with ERP. This finding is in contrast with another study which found comorbid OCPD and OCD to have a greater reduction in the severity of OCD than those without OCPD. Authors suggested that the use of cognitive therapy might have helped in restructuring maladaptive cognitions of OCPD.
Treatment with pharmacological agents also has yielded mixed results in OCD-OCPD comorbidity. In a small study (n = 30), OCPD predicted poorer response to oral serotonin reuptake inhibitors (SRI) at the end of 10 weeks. However, a larger study (n = 55), using clomipramine for 12 weeks failed to find OCPD as the predictor of poorer treatment outcome. Instead, the presence of schizotypal, avoidant and borderline personality disorder (BPD) predicted a significantly poorer outcome.
SCHIZOTYPAL PERSONALITY DISORDER
The prevalence of schizotypal personality disorder (SPD) among OCD patients is found to be as low as 1%. Although the prevalence is low, up to half of OCD patients demonstrate some schizotypal traits.
There is also some overlap in diagnostic criteria of OCRD and SPD [Table 2]. Compared to OCD, the aggressive or sexual obsessions in SPD is not associated with inner resistance. Furthermore, both disorders are associated with magical thinking. Thought-action fusion (TAF) is a negative appraisal which is commonly linked to magical thinking. Among the two major types of TAF, likelihood TAF was associated with schizotypal-magical thinking even after controlling for OC symptoms and negative affect. The authors suggested that an association of likelihood TAF with schizotypy may increase one's chance for OCD.
Neuropsychological studies have preliminary evidence to suggest that OCD-SPD comorbidity might be a distinct subtype. OCD patients when compared to healthy controls were found to have impairment in measures sensitive to the orbitofrontal lobe. However when OCD-SPD patients were compared to healthy controls, deficits were found in both orbitofrontal and dorsolateral prefrontal cortex.
SPD is most consistently found to be a poor predictor of the treatment outcome of OCD both in pharmacotherapy and CBT trials. The schizotypal disorder has predicted treatment failure with both SSRI and clomipramine. In the clomipramine study with 55 OCD patients, three individual criteria of personality disorders which significantly predicted poorer outcome were all from cluster A. These were ideas of reference, odd speech, and paranoid criteria. The poor outcome could be because of the frequent association of schizotypal disorder with poor insight OCD which in itself is a poor prognostic factor. In addition, schizotypal traits are associated with other poor prognostic factors of OCD like an early age of onset, male gender, longer duration of illness, increased severity of OCD, and increased number of comorbidities. Similar findings have also been noted in treatment outcome studies involving CBT. However, there is a some evidence to suggest that comorbid schizotypal disorder may predict response to anti-psychotic augmentation of SSRI.
BORDERLINE PERSONALITY DISORDER
The prevalence of BPD among OCD patients has been estimated to be around 5%. In a cross-sectional study, OCD patients with BPD had higher comorbidity of mood, anxiety and eating disorders; compulsions involving interpersonal domains; greater association with impulsive-compulsive disorders like skin picking disorder; greater mental compulsions; and motor impulsivity. As previously discussed, BPD was associated with poor outcome in one of the pharmacotherapy studies with clomipramine. However, in a larger prospective study with 5-year follow-up, who were treated with either SRI or CBT or a combination of both, BPD was not associated with poor course of illness.
ANXIOUS AVOIDANT PERSONALITY DISORDER
Avoidant personality disorder (AVPD) is the second most common comorbid personality disorder with OCD with prevalence rates ranging from around 5% to 15%. Similar to BPD, the studies have yielded mixed results. Only one pharmacotherapy study with clomipramine has found AVPD to have a poor outcome, whereas the other two larger studies failed to demonstrate such a finding.
AVPD might pose a significant barrier in “collaborative empiricism” of CBT. Due to their fear of rejection, they might fail to involve in therapy adequately or avoid therapy altogether. In such cases, the therapist can see it as an opportunity to elicit automatic thoughts and cognition behind the avoidance and help the patients to test it out.
DEPENDENT PERSONALITY DISORDER
Dependent personality disorder (DPD) is also found to be a common comorbidity with OCD with a prevalence rate of 7.6%. It is characterised by a need to be taken care of and need to seek advice and reassurance from caregivers. Such reassurance seeking is also seen in OCD but is usually restricted to particular symptom dimensions.
The comorbidity of DPD and OCD might pose a challenge in CBT as they might not be receptive to reducing the reassurance seeking, family accommodation and proxy compulsions. There has been a couple based program to enhance ERP involving partner-assisted exposure, reducing maladaptive relationship patterns etc., with a fair degree of success.
Finally, studies which have investigated the presence of unspecified comorbid personality disorders have been inconclusive. The simultaneous occurrence of two or more personality disorders along with OCD has been consistently associated with a negative effect on treatment outcome.
Conclusions
Comorbid personality psychopathology is not uncommon in OCD. Personality disorders affect treatment outcomes of both pharmacological and psychological treatments. It is therefore imperative that treatment plans for such group of patients be individualized and tailor-made to address the issues posed by comorbidity.
References available in original article in Indian Journal of Psychiatry.