“Not just right experiences”: perfectionism, obsessive–compulsive features and general psychopathology
Originally published by: ScienceDirect
Individuals with obsessive–compulsive disorder (OCD) frequently report uncomfortable sensations of things not being just right (“not just right experiences”; NJREs) and a need to ritualize until they quiet these sensations. However, very little work has been conducted to empirically examine the nature and characteristics of this phenomenon. In this paper, we present two studies that systematically examine NJREs in large undergraduate samples. In Study 1, NJREs were shown to be related to both OCD features and maladaptive domains of perfectionism. In Study 2, NJREs were again significantly related to OCD features. Further, NJREs were shown to have particularly strong relationships with specific OCD symptom clusters (e.g., checking, ordering). Finally, NJREs were significantly more strongly correlated with features of OCD than symptoms from other domains of psychopathology (e.g., social anxiety, trait anxiety, worry, depression). General conclusions are drawn, and future directions are discussed. © 2002 Elsevier Science Ltd. All rights reserved.
1. Introduction
Individuals with obsessive–compulsive disorder (OCD) frequently report uncomfortable sensations of things not being just right. Further, these individuals often report feeling driven to perform an action until this uncomfortable sensation can be reduced, to achieve a sensation of things being “just right”. Indeed, Rasmussen and Eisen (1992, p. 756) state that many of their patients with OCD describe “an inner drive that is connected with a wish to have things perfect, absolutely certain, or completely under control”. Until this sense of perfection is achieved, patients may be plagued with a “not just right experience” (NJRE).
Clinicians have long observed NJREs among clients with OCD. In 1903 Janet wrote of “an inner sense of imperfection” and described the experience as follows: “they feel that actions that they perform are incompletely achieved, or that they do not produce the sought-for satisfaction” (in Pitman, 1987b, p. 226). More recent theorists have also discussed feelings of things not being just right or sensations of imperfection. For example, the cybernetic model of OCD (Pitman, 1987a) is based on control systems theory, which treats behavior as a process of matching perceptual input to internal reference signals. The cybernetic model proposes that the core problem in OCD is a mismatch between the perceptual input and internal reference signals (i.e., expectations). Further, it proposes that repetitive and stereotyped behaviors (i.e., compulsions) result from efforts to reduce these mismatch signals. Contemporary cognitive behavioral models (e.g., Rachman, 1997) view many manifestations of OCD as characterized by catastrophic misinterpretations of thoughts. Just as research has shown that most people sometimes experience intrusive thoughts (Rachman & de Silva, 1978), it is also likely that most people sometimes experience NJREs, or mismatches between input and expectations. Further, in both cases (intrusive thoughts and NJREs), the interpretations of these experiences may vary considerably between individuals and dictate their emotional response. If these experiences are interpreted as catastrophic, the result would likely be anxiety.
Despite its presence in the theoretical and clinical literature on OCD, there have been very few attempts to directly measure the phenomenon of NJREs. One research group that has devoted attention to this endeavor is that of Leckman and colleagues, who have conducted a number of studies examining “just right” perceptions (and, by implication, not just right perceptions as well) in individuals with OCD (with and without comorbid tic disorders; Cohen & Leckman, 1992; Leckman, Walker, & Cohen, 1993; Leckman, Walker, Goodman, Pauls, & Cohen, 1994; Leckman et al., 1995; Miguel et al., 2000). They have asked patients a series of questions concerning just right experiences: whether they have ever been or were currently aware of a need to perform compulsive acts until they are “just right”, whether this awareness was more mental or physical in nature, and at what particular moment (before starting, or during, compulsions) they became aware of the need for things to be “just right”. Leckman et al. (1994) found that a large proportion of 177 individuals with OCD (with or without a comorbid tic disorder) reported the occurrence of just right perceptions at some point in their illness (92%) and many reported the occurrence of just right perceptions during the past week (73%). Further, the occurrence of just right experiences was positively related to the severity of OCD features, with those reporting the occurrence of just right experiences in the past week having more severe symptom ratings. Individuals with OCD with and without a comorbid tic disorder were not found to differ on the occurrence of just right experiences. In a more recent study, 63% of 40 individuals with OCD with or without Tourette’s Disorder endorsed repetitive behaviors preceded by feelings of things not being just right (Miguel et al., 2000).
While the work of Leckman’s group has been groundbreaking, these studies are limited in a number of ways. First, their measure was a single item dichotomously reporting the presence or absence of just right perceptions. This method of measurement is unlikely to be sensitive and may present only a crude indication of the presence or impact of NJREs. Second, these studies were conducted solely in clinical samples, and it is important to determine whether NJREs occur in non-clinical samples as well. Comparisons of NJREs reported by persons with OCD and by non-anxious persons is particularly important given findings that most individuals experience obsessions, but that clinical and non-clinical samples can be distinguished by the frequency and other characteristics of the obsessions (e.g., duration, intensity, and consequences; Rachman & de Silva, 1978). Third, previous studies of NJREs have not addressed the possible relationship between NJREs and perfectionism. This is an important area for study, as some authors have proposed that NJREs may represent a specific form of “sensation-based perfectionism” that has a unique relationship with OCD. For example, Pitman (1987a) proposed that many perfectionistic OCD behaviors are attempts to match sensations with expectations. To date, empirical studies of perfectionism (mainly focusing on evaluation of performance) and OCD have failed to find specific types of perfectionism that distinguish OCD from other disorders (for a review, see Frost, Rhe ́aume, & Novara, 2002). However, whether sensory perfectionism, in the form of NJREs, represents a form of perfectionism specific to OCD has not yet been empirically examined.
Other empirical studies have addressed NJREs less directly than Leckman’s group. NJREs and sensations of imperfection have frequently been discussed in empirical work on subgroups of individuals with OCD (e.g., Calamari, Wiegartz, & Janeck, 1999) and groupings of OCD symptoms (e.g., Baer, 1994; Summerfeldt, Richter, Antony, & Swinson, 1999). For example, in explaining why their “certainty” subgroup had more severe symptoms than the four other clusters on various measures of checking, doubting, and slowness, Calamari et al. (1999) argued that these findings were consistent with “this subgroup’s core concerns involving a need to be absolutely certain to prevent a negative outcome or certainty for the sake of knowing or producing a just right feeling unrelated to outcome” (pp. 122–123, emphasis added). Summerfeldt et al. (1999) found that symmetry obsessions with and without magical thinking displayed substantially different magnitudes of relationship with a symmetry and exactness factor (r = 0.25 and 0.48, respectively). Based on clinical observation, Summerfeldt et al. (1999) argued that, despite their overt similarity, obsessions with and without magical thinking are distinct. They proposed that this is primarily due to disparate motivations, specifically “harm avoidance in the case of symmetry obsessions with magical thinking versus a need to have things ‘just right’ in the case of those without” (p. 308). Finally, in his identification of symptom subtypes in OCD, Baer (1994) noted that the largest factor in his factor analysis of the Yale–Brown Obsessive Compulsive Scale (Y-BOCS) Symptom Checklist, symmetry/hoarding, was composed of symptoms reminiscent of Janet’s description of patients who are bothered by an inner sense of imperfection.
1.1. The current studies
In summary, while NJREs have been frequently noted by OCD theorists and frequently observed both clinically and in empirical work, there have been only limited attempts to directly measure the phenomenon and study its role in OCD. The studies presented herein sought to further examine the nature of NJREs and their relationships to other variables of importance in large non-clinical samples. Study 1 examined the relationship of NJREs to features of OCD and domains of perfectionism. Study 2 examined the relationship of NJREs to various types of OCD features and other domains of psychopathology.
2. Study 1
The sample consisted of 119 female introductory psychology students who received course credit for participating. Participants were freshman and sophomores at a small private liberal arts college for women. The ethnic composition of the college was predominantly Caucasian, and the majority of students came from middle to upper class socioeconomic backgrounds.
2.1. Measures
2.1.1. NJRE-Questionnaire (NJRE-Q)
The NJRE-Q begins by defining NJREs as “times when you have the subjective sense that something isn’t just as it should be”. Further NJREs are defined as having their roots in the individual, i.e., an unsettled feeling because something in the individual or in their perception that the world around them is not right. After the definition and a series of examples, 13 NJREs are presented (see Fig. 1), and respondents are asked to report whether they had this experience in the past week or ever. The 13 NJREs were developed based on clinical experience, input from clients with OCD, suggestions from individuals with OCD via the internet, and pilot work. Efforts were made to include NJRE situations that were not from typical domains of OCD concerns to avoid complete overlap with OCD symptom content. After rating the occurrence of the 13 NJREs, respondents then identified which NJRE had occurred most frequently in their life and rated it on 22 additional dimensions. These ratings examined frequency (two items), intensity (four items), importance (five items), and anxiety (six items). For each of these sets of items, we calculated an average item score by summing the scores for all items and then dividing this total by the number of items in the set. A single question asked respondents to indicate whether the NJRE was (a) more like a mental awareness, (b) more like a body feeling, (c) both a mental awareness and a body feeling, or (d) more like something else. Another item asked respondents what they said to themselves when they experienced the feeling: (a) nothing, (b) that it was a strange experience without any importance, or (c) that it must mean there was something wrong or incomplete. One item assessed the degree to which the respondent believed that things needed to be perfect (from 0 = not at all to 4 = extremely strong). Another item assessed what participants did in response to the sensation: (a) nothing, left it alone, (b) distracted myself, (c) started worrying about it, (d) concretely did some action to correct it, or (e) did something else _ . And, finally, one item asked respondents to indicate to what extent they believed that a bad mood at the time (e.g., feeling down, anxious or irritable) had something to do with the NJRE (from 0 = not at all to 4 = totally).

Fig. 1. NJREs presented in the NJRE-Q used in Study 1.
2.1.2. Padua Inventory (PI)Paragraph
The original PI (Sanavio, 1988) is a 60-item self-report inventory assessing four factors related to obsessive–compulsive behavior: impaired mental control, checking, loss of control of actions, and contamination. Each item is rated from 0 = not at all disturbing to 4 = very much disturbing. Sanavio (1988) found the PI to have good psychometric properties, including strong internal consistency (∝ = 0.90 for males, 0.94 for females) and good 30-day retest reliability (r = 0.78 for males, 0.83 for females). Finally, the PI total score has been shown to discriminate individuals with OCD from individuals with neurotic disorders (Sanavio, 1988). Since the publication of the original version of the PI, many other versions have also been used. For example, the 39-item PI–Washington State University Revision (Burns, Keortge, Formea, & Sternberger, 1996), the 41-item Padua Inventory–Revised (van Oppen, Hoekstra, & Emmelkamp, 1995), and the 40-item abridged version (Rhe ́aume et al., 2000). The 40-item abridged version was used in the current study.
2.1.3. Multidimensional Perfectionism Scale (MPS)
The MPS (Frost, Marten, Lahart, & Rosenblate, 1990) is a 35-item self-report scale developed based on a multidimensional conception of perfectionism. The scale is composed of six subscales: (1) concern over mistakes, (2) doubts about actions, (3) personal standards, (4) parental expectations, (5) parental criticism, and (6) organization. An overall perfectionism score can also be calculated by summing all items except those from the organization subscale. Frost et al. (1990) found internal consistency to be excellent (∝ = 0.90) for the overall perfectionism score and to range from good to excellent for the subscales (∝ = 0.77 to 0.93). Further, the overall perfectionism score was significantly correlated with other measures of perfectionism.
2.1.4. Perfectionism Questionnaire (PQ)
The PQ (Rhe ́aume, Freeston, & Ladouceur, 1995) was developed based on a unidimensional conception of perfectionism and is intended to distinguish between functional and dysfunctional perfectionism. The scale is composed of 64 ratings across four different domains. The perfectionistic tendencies scale (10 items) assesses the degree to which one has high personal standards and feels an inner drive to strive for perfectionism. The domains scale (22 items) assesses the extent to which the respondent is perfectionistic across various domains of his or her life, such as work, studies, and health. The demandingness scale (8 items) assesses how demanding the respondent is towards various groups of people such as his or her children, colleagues, and strangers. Finally, the disadvantages subscale (24 items) assesses the negative consequences of perfectionism such as stress, discomfort, and avoidance. The PQ has been shown to have good construct validity in a sample of 800 university students. The subscales of the PQ also have demonstrated good internal consistency (based on three subscales, collapsing the domains and demandingness subscales above into one domains subscale: perfectionistic tendencies ∝ = 0.82, domains affected by perfectionistic behavior ∝ = 0.88, and negative consequences of perfectionism a 0.96) (Rhe ́aume et al., 2000).
2.2. Results
2.2.1. Scale characteristics
To examine how well the occurrence ratings for the 13 NJREs held together, we computed indices of the internal consistency of these scales using the Kuder–Richardson Formula #20 (KR-20). These analyses revealed that the 13 items held together fairly well (past week ∝ = 0.57, ever ∝ =0.64). We also examined the cohesiveness of the items assessing the four domains of associated features of the NJREs. These analyses revealed strong cohesiveness of the items: frequency scale ∝ = 0.93, intensity scale ∝ = 0.86, importance scale ∝ = 0.76, and anxiety scale ∝ = 0.86.
2.2.2. Prevalence and nature of NJREs
Focusing first on NJREs experienced within the past week, 95% of the sample reported having experienced at least one of the 13 NJREs. The percentage of participants reporting specific NJREs within the past week ranged between 9% and 51% [mean (M) = 27%]. The NJRE most commonly reported in the past week was “When setting the alarm, I have had the feeling it wasn’t done just right”. Turning to NJREs experienced at any time in the participants’ lives, 99% of the sample reported having ever experienced at least one of the 13 NJREs. The percentage of participants reporting specific NJREs at any time in their lives ranged between 44% and 69% (M = 59%). The NJRE most commonly reported as having ever occurred was “I have had the inexplicable feeling that something bad or out of the ordinary was about to happen”.
To better understand the characteristics of these NJREs, we then examined the mean scores for the associated ratings (e.g., intensity, importance, etc.). All ratings were made on a scale from 0 (indicating the minimal level of that symptom) to 4 (indicating the maximum level of that symptom). For the frequency items, 0 indicated never and 4 indicated once a day or within the past day. The average item score for the frequency scale was 3.23 [standard deviation (SD) = 0.73], suggesting that respondents experienced NJREs almost daily. The average item score for the intensity scale (M = 1.35, SD = 0.87) revealed that participants reported experiencing between “a little” and “moderate” intensity/distress associated with the NJRE. Regarding importance, the average item score (M = 1.31, SD = 0.77) revealed that participants attributed “a little” to “moderate” importance to the NJRE. Finally, participants reported nearly moderate anxiety (M = 1.86, SD = 0.92) associated with the NJRE.
Regarding the mental vs. physical nature of the sensations, 62.2% of participants reported that their most frequent NJRE was “more like a mental awareness”, 29.4% reported the experience as “both a mental awareness and a body feeling”, and only 7.6% reported the experience as “more like a body feeling”. Regarding what respondents said to themselves when they experienced the feeling, 49.1% responded “that it must mean there was something wrong or incomplete”, 27.6% responded that they said “nothing”, and 23.3% responded that they said “that it was a strange experience without any importance”. In response to the NJRE experience, 52.1% of participants reported that they “concretely did some action to correct it” whereas only 16.8% reported that they did “nothing”. The item assessing the degree to which the respondent believed that things needed to be perfect revealed that participants responses averaged to a level between “1 = a little strong” and “2 = moderately strong” (M = 1.82, SD = 1.17). And, finally, the response to an item assessing the extent to which respondents believe that a bad mood at the time had something to do with the NJRE revealed that participants’ responses averaged to a level between “1 = a little” and “2 = moderately” (M = 1.32, SD = 1.30).
2.2.3. Relationship of NJREs to OCD features
To examine the relationship of NJREs to OCD features, we correlated NJRE ratings with the total and subscale scores of the PI (see Table 1). First, we correlated the total number of NJREs in the past week (total NJREs PW) and the total number of NJREs endorsed as having ever occurred (total NJREs ever) with the PI. The total NJREs PW was significantly correlated with the PI total score and all subscale scores. However, the correlation of total NJREs PW with the PI contamination subscale was much smaller in magnitude [r(119) = 0.29, P < 0.001] than the correlation of total NJREs PW with the other subscales (r = 0.41 to 0.46) and significantly smaller than its correlation with the PI total score [r(119) = 0.49, P < 0.001; test of dependent correlations, z = 3.32, P < 0.001]. Interestingly, total NJREs ever showed negligible correlations with the PI total or subscale scores (r = 0.04 to 0.20). In further contrast to the findings for the past week, total NJREs ever was found to be significantly correlated only with the PI contamination subscale at an alpha level of 0.05 [r(119) = 0.20, P = 0.026], although the magnitude of this correlation was small.
Given the apparent discrepancy in the magnitude of correlations for the total NJREs in the past week as compared to ever, we decided to test whether the magnitude of these correlations differed significantly. To this end, we conducted tests of dependent correlations comparing the correlations of the two NJRE total scores with the PI total and each of the four PI subscales. Indeed, the PI total score and three of the four subscales (all except contamination; z = 0.74, P = 0.23) were significantly more strongly correlated with the total NJREs in the past week than with the total NJREs ever.

Table 1
Study 1: Scale ranges, means (M), standard deviations (SD), and correlations of NJRE ratings with measures of OCD features and perfectionism
N = 119.
∗P < 0.05.
∗∗P < 0.01.
∗∗∗P < 0.001.
Next, we correlated the associated NJRE ratings, including the four average item scores, with the PI. As can be seen in Table 1, all four average item scores were significantly correlated with the PI total score (r = 0.34 to 0.45). Examination of the PI subscale scores revealed that all four average item scores were significantly correlated with the impaired mental control, checking, and loss of control of actions subscales (r = 0.23 to 0.45). However, only the NJRE frequency average item score was shown to be significantly correlated with the contamination subscale of the PI [ r(119) = 0.20, P < 0.05]. Of the individual items rating associated features of the NJREs, the item that was most strongly correlated with the PI total score was the item assessing the extent to which the NJRE interfered with ongoing activities [r(119) = 0.44, P < 0.001].
2.2.4. Relationship of NJREs to domains of perfectionism
To examine the relationship of NJREs to domains of perfectionism, we correlated the NJRE scores with the two measures of perfectionism (see Table 1). First, we correlated total NJREs PW and total NJREs ever with the MPS and PQ. Total NJREs PW was significantly correlated with all subscales and the overall perfectionism score of the MPS (r = 0.19 to 0.40). Total NJREs PW was also significantly correlated with all four subscales of the PQ (r = 0.22 to 0.42). Of these four subscales, total NJREs PW was most strongly correlated with the disadvantages subscale, which assesses the negative consequences of perfectionism. Once again, we found much weaker relationships for total NJREs ever. Indeed, of all the subscales of the MPS and the PQ along with the MPS overall perfectionism score, total NJREs ever was only significantly correlated with the PQ domains of perfectionism subscale. Although statistically significant, this correlation was modest [r(119) = 0.21, P < 0.03].
Next, we correlated the four NJRE average item scores with the two measures of perfectionism. The intensity, importance, and anxiety domains for the NJREs were significantly correlated with the MPS overall perfectionism score (see Table 1). Examination of the subscales of the MPS revealed the strongest correlations for the intensity and importance of NJREs with the concern over mistakes, doubts about actions, and personal standards subscales (r = 0.32 to 0.46). While various other correlations were significant, they were all weaker in magnitude (all other correlations were < 0.30). The intensity and importance of the NJREs showed the strongest correlations with the PQ subscales. Indeed, the intensity and importance ratings showed significant relationships with all four subscales of the PQ (r = 0.25 to 0.41). The anxiety ratings for the NJREs showed significant, but weaker, correlations with the four PQ subscales (r = 0.20 to 0.24). Finally, the frequency ratings for the NJREs were not significantly related to any PQ subscales (r = 0.03 to 0.17).
2.3. Discussion
What conclusions can be drawn from this first study? First, unselected students experience NJREs. Indeed, the large majority of participants (95%) endorsed having experienced at least one of the NJREs presented within the past week, and nearly all participants (99%) reported having experienced at least one of the NJREs at some time. Second, these results provide support for a significant relationship between NJREs and OCD. Both the occurrence of NJREs within the past week and the experiences associated with these NJREs (intensity, importance, and anxiety) were related to overall levels of OCD features. Further, an examination of types of OCD features revealed that NJREs may be more strongly related to some types of OCD symptoms than others. For example, the NJRE ratings were more strongly related to control and checking features of OCD than to contamination concerns. Finally, there was also a meaningful relationship between NJREs and perfectionism. More specifically, the occurrence of NJREs within the past week and the intensity and importance of these NJREs were meaningfully related to maladaptive domains of perfectionism (e.g., concern over mistakes, doubts about actions, and disadvantages of perfectionism).
One notable finding was the striking difference between results for the total NJREs experienced in the past week versus the total NJREs ever experienced. For all correlations with measures of OCD features and perfectionism, total NJREs PW showed a stronger correlation than total NJREs ever. Indeed, the magnitude of correlations for total NJREs ever were generally negligible (r = 0.00 to 0.21), whereas those for total NJREs PW were generally of moderate magnitude (r = 0.19 to 0.49). These findings are particularly important as this is the first study to examine NJREs in a non-clinical sample. Further, it appears that the interpretation of the intensity and importance of these experiences, and not their frequency, is related to the presence of OCD symptoms. Indeed, the intensity and importance ratings (not frequency) showed the highest correlations with levels of OCD features. Consistent with cognitive–behavioral models of OCD (Rachman, 1997), our findings suggest that it is not merely the presence or absence of NJREs that is relevant to OCD, but instead that it is the interpretations of these experiences (e.g., interpretations of intensity and importance). These findings are also consistent with the findings of Rachman and de Silva (1978) that normal obsessions are common and that they resemble abnormal obsessions in both form and content. However, normal and abnormal obsessions differ in duration, intensity, and consequences.
Our findings regarding the relationship of NJREs to OCD features are clearly consistent with existing models and previous empirical work. It is also worthwhile to briefly consider how our findings regarding perfectionism and NJREs fit with previous work that has examined the relationship between perfectionism and OCD. Two studies with non-clinical samples have found Concern over Mistakes and Doubts about Actions to be positively correlated with total scores on self-report measures of OCD features (Frost et al., 1990; Rhe ́aume, Freeston, Dugas, Letarte, & Ladouceur, 1995). These findings are notably similar to the relationships found in the current study between the subscales of the MPS and the occurrence of NJREs. Specifically, in the current study, the total NJREs PW was most strongly correlated with the Doubts about Actions subscale followed by the Concern over Mistakes subscale.
Finally, it is important to consider the limitations of this first study. Although the sample was large (N = 19), the generalizablility of the findings is limited by the homogeneous nature of the sample (unselected female undergraduates). Studies employing more heterogeneous samples (e.g., individuals of both genders, from more varied ethnic backgrounds, and both with and without OCD) would serve to increase generalizability. Another limitation is that the measure of OCD features represented only limited content domains. A more comprehensive measure of OCD features would allow for further examination of the relationship of NJREs to specific types of OCD features. And, finally, other domains of psychopathology (e.g., depression, social anxiety) were not examined in this study, thereby limiting conclusions regarding the specificity of the relationship between NJREs and OCD features in particular.
3. Study 2
One question not adequately addressed by the first study is whether NJREs are differentially related to specific types of OCD features. First, based on the work of Summerfeldt et al. (1999) and Baer (1994), we predicted that NJREs would be strongly correlated with symptoms of symmetry or ordering. Second, based on the discussion of Calamari et al. (1999), we predicted that NJREs would be strongly correlated with checking and doubting. To test these hypotheses, Study 2 used a different measure of OCD features that provides a more comprehensive profile of OCD features than the PI used in Study 1. Further, in addition to the benefits of the subscales of this new measure of OCD features, use of this scale’s total score allowed us to replicate the findings of a relationship between OCD features and NJREs found in Study 1.
Another important question not answered by Study 1 is whether NJREs represent a specific form of perfectionism that has a unique relationship to OCD features. As discussed in the Introduction, previous studies have failed to demonstrate a unique relationship between specific forms of perfectionism and OCD. Previous studies have shown various domains of perfectionism (e.g., doubts about actions, concern over mistakes) to be related to OCD, but these same domains have also been shown to be related to many other forms of psychopathology (see Frost et al., 2002). Therefore, the lack of specificity of this relationship has limited the utility of these findings. However, NJREs may represent a specific form of perfectionism that characterizes features of OCD, and Study 2 was designed to examine the specificity (discriminant validity) of the NJRE phenomenon. We included measures of various other forms of psychopathology (e.g., trait anxiety, worry, depressive symptoms, social anxiety) that could reasonably be related to NJREs but that were predicted to show weaker correlations with NJREs than would OCD features.
In addition, we utilized information gathered in Study 1 to refine and streamline our measure of NJREs. First, the questionnaire was revised to ask respondents to rate the occurrence of specific NJREs within the past month, instead of in the past week and ever. This change was guided by the findings of Study 1 that total NJREs PW was more strongly correlated with OCD features and domains of perfectionism than total NJREs ever. Therefore, for the revised questionnaire, we decided to use a discrete amount of time, but broadened the duration slightly (increased from one week to a month) to avoid situational fluctuations that may occur in the very short period of a week. Second, the number of associated ratings performed for the targeted NJRE was significantly reduced. In the revised form, respondents make seven associated ratings for the most recent NJRE (compared to 22 in Study 1). The content of these ratings was guided by the findings of Study 1 and attempts to measure the key aspects of the NJREs while avoiding redundant items.
Finally, in Study 2, data were gathered from a more diverse sample. The sample for Study 2 consisted of 242 introductory psychology students who participated in partial fulfillment of course requirements. Their age ranged from 17 to 47 years, with a mean of 19.73 years (SD = 3.17). Most students (226) were single, two were married, three reported living with partners, one was divorced, one was separated, and the remainder failed to report marital status. As in Study 1, the majority of participants were freshmen (n = 121) and sophomores (n = 67), along with some juniors (n = 36), and 18 others. In contrast to Study 1, participants in the current study represented both genders (161 females, 75 males, and six participants who did not report gender). Participants were also from diverse ethnic backgrounds. Of the 212 participants reporting race, 85 were of European descent, 59 were African–American, 26 were Asian or Asian–American, 12 were Hispanic, and 30 reported mixed heritage.
3.1. Measures
3.1.1. Revised NJRE Questionnaire (NJRE-QR)
The NJRE-QR is a 19-item self-report questionnaire. The first 10 items present sample NJREs (see Fig. 2) and ask respondents to indicate whether or not they experienced each NJRE within the past month. After rating the occurrence of each NJRE, respondents are asked to indicate which NJRE occurred most recently and when it last occurred (from within past few hours to within past month). Then, thinking of that particular NJRE, respondents are asked to complete seven ratings (see Table 2).
3.1.2. Obsessive Compulsive Inventory (OCI)
The OCI (Foa, Kozak, Salkovskis, Coles, & Amir, 1998) is a 42-item self-report measure of obsessive features. Each item is rated on 5-point (0–4) Likert-type scales for (a) the frequency of the symptom, and (b) the severity of the associated distress. Individuals with OCD have been shown to have significantly higher OCI distress and frequency total scores than individuals with social phobia or post traumatic stress disorder, and controls (Foa et al., 1998). Further, OCI scores are strongly correlated with other self-report measures of obsessive features (r = 0.65 to 0.81). Internal consistency for the full scale is good (∝ = 0.86 to 0.95), and both the distress and frequency total scores have demonstrated good retest reliability in both OCD and control samples (r = 0.84 to 0.90). Further support for the strong psychometric properties of the OCI in undergraduate samples is provided by Simonds, Thorpe, and Elliott (2000).
3.1.3. Beck Depression Inventory (BDI)
The BDI (Beck, Rush, Shaw, & Emery, 1979) is a 21-item self-report scale, which focuses primarily on the cognitive symptoms of depression. Each item is rated on a scale of 0 to 3 with higher scores indicative of greater severity. The BDI exhibits good internal consistency in both psychiatric and non-psychiatric samples (mean ∝ = 0.86 and 0.81, respectively) and good concurrent validity with other measures of depression (Beck, Steer, & Garbin, 1988). For a detailed discussion of the use of the BDI over the past 25 years, see Beck, Steer, et al. (1988)).

Fig. 2. NJREs presented in the NJRE-QR used in Study 2.

Table 2
Study 2: Means (M) and standard deviations (SD) for the associated ratings performed on the NJRE-QR and correlations of these ratings with the OCI frequency and distress total scores
All ratings shown ranged from 1 to 7, with 1 indicating absence of that symptom to 7 indicating extreme levels of that symptom (e.g., 1 = not intense at all to 7 = extremely intense). For the frequency item, 1 indicated never and 7 indicated within the past day.All correlations P < 0.001.
3.1.4. State-Trait Anxiety Inventory-Trait form (STAI-T)
The STAI-T (Spielberger, Gorsuch, Lushene, Vagg, & Jacobs, 1983) is a 20-item self-report measure of the tendency to perceive stressful situations as dangerous or threatening and the tendency to respond to these situations with increases in state anxiety. Participants are asked to rate each item on a 4-point Likert-type scale from 1 (“almost never”) to 4 (“almost always”) to indicate how they generally feel. Retest reliability for the STAI-T has been shown to be high, ranging from 0.73 to 0.86, and validity correlations with other anxiety questionnaires range from 0.73 to 0.85 (Spielberger et al., 1983).
3.1.5. Beck Anxiety Inventory (BAI)
The BAI (Beck, Epstein, Brown, & Steer, 1988) is a 21-item self-report measure of anxiety symptoms developed to improve discrimination between symptoms of depression and anxiety. The BAI instructs participants to rate each item as to how much the symptom has bothered them in the past week. Ratings are made on a scale from 0 = not at all to 3 = severely. The BAI has been shown to have high short-term retest reliability and internal consistency (Beck, Epstein, et al., 1988) as well as strong convergent and discriminant validity (Fydrich, Dowdall, & Chambless, 1992). In a large undergraduate sample (N = 326), Creamer, Foran, and Bell (1995) found the BAI to have strong internal consistency (∝ = 0.91). Retest reliability over a period of approximately a month was shown to be modest (r = 0.62), consistent with the conceptualization of the BAI as a state measure.
3.1.6. Brief Fear of Negative Evaluation Scale (B-FNE)
The B-FNE (Leary, 1983) is a 12-item self-report inventory designed to assess cognitions that characterize social anxiety. The B-FNE is distinguished from the original FNE scale (Watson & Friend, 1969) in two main ways: (1) it contains 12 items while the original scale contains 30, and (2) item ratings for the B-FNE are made on a Likert-type scale from 1 (“not at all characteristic of me”) to 5 (“extremely characteristic of me”), whereas item ratings for the original scale are made using a true–false format. The B-FNE has been shown to have excellent inter-item reliability (∝ = 0.92) and retest reliability (r = 0.75; Elting & Hope, 1995). The brief and full versions of the FNE are highly correlated (r = 0.96; Leary, 1983).
3.1.7. Penn State Worry Questionnaire (PSWQ)
The PSWQ (Meyer, Miller, Metzger, & Borkovec, 1990) is a 16-item self-report inventory designed to assess trait worry and to capture the generality, excessiveness, and uncontrollability characteristic of pathological worry (e.g., “My worries overwhelm me”; “I worry all the time”). Each item is rated on a 1 (“not at all typical of me”) to 5 (“very typical of me”) Likert-type scale. In undergraduate samples, the PSWQ has repeatedly demonstrated good internal consistency and good retest reliability over intervals as long as 8–10 weeks (Meyer et al., 1990). Individuals with a principal diagnosis of Generalized Anxiety Disorder (GAD) have been shown to score higher on the PSWQ than community controls and patients with panic disorder, panic disorder with agoraphobia, social phobia, simple phobia, or OCD (Brown, Antony, & Barlow, 1992). Molina and Borkovec (1994) provide a more detailed review of the psychometric properties of the PSWQ.
3.2. Results
3.2.1. Scale characteristics
To examine the cohesiveness of the 10 items assessing the occurrence of NJREs, we computed the internal consistency of the scale using the KR-20 Formula. This revealed that the 10 NJREs presented had strong internal consistency (∝ = 0.79). Further, there were no cases in which deletion of an item would improve the internal consistency of the scale. Therefore, we computed a total score for the occurrence of the NJREs to use in subsequent analyses.
3.2.2. Prevalence and nature of NJREs
Eighty per cent of the sample reported having experienced at least one of the 10 NJREs within the past month. The mean number of NJREs endorsed as having occurred within the past month was 3.26 (SD = 2.7). The percentage of participants reporting specific NJREs within the past month ranged from 18% to 54% (M = 33%). The most frequently endorsed NJRE was “When talking to people, I have had the sensation that my words did not sound just right”, and the least frequently endorsed NJRE was “When putting a bill or letter into a mailbox, I have had the sensation that the way I placed the envelope in the mailbox and closed the door didn’t feel just right”.
3.2.3. Ratings of characteristics of NJREs
In addition to reporting the occurrence of NJREs within the past month, participants also completed a series of ratings for the NJRE that they had experienced most recently (see Table 2). As a whole, these ratings tended to be low. This suggests that while these college students did experience NJREs, on average, they were not associated with much distress or other aversive experiences. However, as can be seen by an examination of the standard deviations, there was variability in the ratings, suggesting that some individuals may experience higher levels of associated symptoms.
We also examined the relationship of these ratings to OC features (see Table 2). Each item was correlated with the OCI frequency and distress totals. Overall, these correlations were generally in the moderate range (r = 0.27 to 0.44). Due to the small amount of variability in the magnitude of these correlations, we did not test their statistical difference. However, it may be worth noting that the item assessing the frequency of the NJRE consistently showed the smallest magnitude of correlation with the OCI totals.
3.2.4. Relationship of NJREs to types of OCD features
We also sought to examine whether the occurrence of NJREs was differentially related to various types of OC features. To examine this question we correlated the NJRE total score with the seven subscales of the OCI (see Table 3). These correlations of NJREs to types of OCD features were all moderate to strong in magnitude (r = 0.44 to 0.60). Based on previous work, we had predicted that the checking, ordering, and doubting subscales would show particularly strong correlations with NJREs. Visual examination of the correlations revealed that, of the OCI subscales, the checking subscale consistently showed the strongest correlations with NJREs. The ordering and doubting subscales were also consistently among the top three or four largest correlations between NJREs and subscales of the OCI.
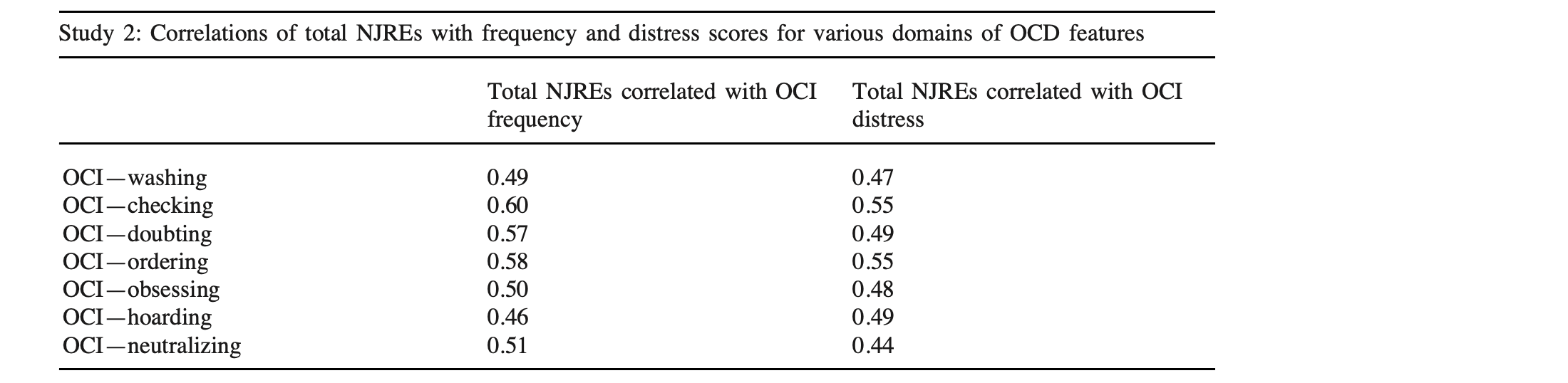
Table 3
Study 2: Correlations of total NJREs with frequency and distress scores for various domains of OCD features
OCI, Obsessive Compulsive Inventory.
To test the statistical significance of differences between the correlations we computed a composite correlation for each type of OCD symptom. This was calculated by combining the two correlations for each OCI subscale (frequency and distress) via Fisher Z transformations. We then compared the magnitude of these composite correlation coefficients for various domains of OCD features. Based on our predictions we tested whether the correlation of NJREs with the checking composite score was significantly larger than correlations of NJREs with domains of OCD features that have not been frequently discussed in the literature on NJREs (washing, obsessing, hoarding, neutralizing). The correlation of NJREs with the checking composite score (frequency and distress of checking) was found to be significantly larger than the correlations of NJREs with the washing, obsessing, hoarding, and neutralizing composite scores (all P < 0.02). The composite ordering correlation was also found to be significantly more strongly correlated with total NJREs than was washing, obsessing, hoarding, or neutralizing (all P < 0.05). The correlation of NJREs with the doubting composite score was not shown to be significantly larger than the correlations of NJREs with the composite washing, obsessing, or hoarding scores (all P > 0.10), but did show a trend towards being larger than the correlation with neutralizing (P = 0.09).
3.2.5. Relationship of NJREs to OCD features vs. relationship to other forms of psychopathology
To examine the specificity of NJREs to OCD, we compared the relationships of the NJRE total scores with measures of OC features to their relationship with the measures of other domains of psychopathology (trait anxiety, worry, social anxiety, depressive symptoms). As can be seen in Table 4, total NJREs was strongly correlated with both total scores of the OCI. Further, total NJREs remained significantly correlated (all P < 0.001) with both the frequency and distress of OCD symptoms when controlling for levels of trait anxiety (controlling for STAI-T, r = 0.58 and 0.51, respectively; controlling for BAI, r = 0.54 and 0.43, respectively), worry (r = 0.56 and 0.49, respectively), social anxiety (r = 0.60 and 0.54, respectively), and depressive symptoms (r = 0.57 and 0.50, respectively). Consistent with our predictions, the correlations of the NJRE total score with measures of other domains of psychopathology were weaker (r = 0.21 to 0.45), although significant (all P < 0.01). Tests of dependents correlations revealed that the NJRE total score was significantly more strongly correlated with the OCI total frequency and the OCI total distress scores than with any of the other symptom measures (all P < 0.02).

Table 4
Study 2: Scale ranges, means (M), standard deviations (SD), and correlations with the total NJREs
OCI-F total, Obsessive Compulsive Inventory total frequency score; OCI-D total distress score; BDI, Beck Depression Inventory; STAI-T, State Trait Anxiety Inventory-Trait Form; BAI, Beck Anxiety Inventory; Brief FNE, Brief Fear of Negative Evaluation Scale; PSWQ, Penn State Worry Questionnaire. For the correlations with the OCI totals all P < 0.001, all other correlations P < 0.01.
4. General discussion
What conclusions can be drawn from this second study? First, we again found that a substantial percentage of the sample reported experiencing at least one NJRE within the given time frame (in this case, one month). The percentages of the sample endorsing at least one NJRE were lower than those found in Study 1. However, this may be a result of a more limited set of NJREs to choose from, as Study 2 presented only 10 NJREs in each set and Study 1 presented 13. The current study also replicated our finding of a significant relationship between NJREs and levels of OC features, and went beyond Study 1 in showing that there is specificity in the relationship between total NJREs and the various types of OC features. Consistent with predictions based on previous empirical work, the OC features that tended to show the strongest correlations with NJREs were checking, ordering, and doubting. The symptoms that tended to show weaker correlations with NJREs were washing, obsessing, hoarding, and neutralizing. Finally, the results of Study 2 suggest a unique relationship of NJREs to features of OCD versus other types of psychopathology. NJREs were significantly more strongly correlated with levels of OC features than with several other symptom domains. Thus, NJREs may represent a specific form of perfectionism that has a unique relationship to OC features. This finding stands in contrast to previous studies that failed to demonstrate a unique relationship between perfectionism and OC features.
What can we learn from the differential relationship of NJREs to specific domains of OC features? First, the consistency of our findings with previous discussions linking NJREs to particular domains of OC features lends further credence to the viability and usefulness of measuring NJREs in a self-report format. Our findings are clearly consistent with empirical work on subgroups of individuals with OCD (Calamari et al., 1999) and groupings of OC features (Baer, 1994; Summerfeldt et al., 1999). Our results are also consistent with the findings of Ferrari (1995) that there was a significant positive correlation between perfectionistic cognitions and compulsive checking, but not with compulsive washing. In addition to considering the types of OC features that showed the strongest correlations with NJREs, it is also worthwhile to consider those that showed smaller, but still substantial, correlations. For example, while washing was typically ranked as one of the smaller correlations among the symptom domains, the magnitude of correlations of this subscale with NJREs was not negligible (r = 0.47 and 0.49). Further, it is possible that some of these more modest correlations may have been diminished compared to some of the others because such symptoms may occur for various reasons. For example, washing may be motivated by an attempt to reduce the likelihood of a feared outcome (e.g., washing to remove germs and thereby prevent illness) or motivated by an attempt to achieve a sensation of one’s skin feeling just right (e.g., to remove a tacky or sticky feeling from the hands). This line of thought is consistent with the work of Tallis (1996), who proposes that there are some patients for whom washing is not to remove contamination, but rather to achieve a perfect state of cleanliness. Based on this distinction, Tallis (1996) proposes that the second type of washing may be more closely linked to perfectionism. In summary, it is possible that further precision in distinguishing the motivations behind symptoms may reveal more precise relationships of the various types of OC symptoms and NJREs.
Distinguishing between symptoms motivated to prevent a feared consequence versus those motivated by reducing an NJRE may also have important implications for treatment. Compulsions are typically conceptualized as attempts to reduce anxiety by decreasing the probability of a feared consequence. For example, checking the knob of a stove is commonly conceptualized as an attempt to confirm that the stove is off and thereby prevent a fire. However, these same compulsions could be motivated by a desire to reduce the anxiety caused by NJREs, to decrease a sense of uneasiness that something in the surroundings is out of place at that time. For example, the individual who repeatedly turns the knob of the stove may not necessarily be fearful of a fire, but may need to repeatedly turn it until the position of the knob in their hand “feels right”. Considering the possibility of compulsions as attempts to relieve NJREs may serve to improve therapy outcomes. In fact, Foa, Abramowitz, Franklin, and Kozak (1999) found that OCD patients who did not articulate feared consequences showed a trend towards having higher (i.e., more severe) post-treatment symptom scores than those who had articulated feared consequences. It is possible that those patients who did not articulate feared consequences were distressed by NJREs. In other words, experiencing the NJRE was their feared consequence. While typical exposures are likely to elicit NJREs in such clients, specifically designing exposure exercises with the goal of eliciting an NJRE may improve outcomes.
What are the next steps? First, it will be important to conduct empirical work examining the NJRE phenomenon in clinical samples. These findings should then be compared to those from non-clinical samples. Second, it is important to further assess whether the construct of NJREs is separable from other constructs such as obsessional doubting, obsessions, or OCD symptoms more broadly. It is reasonable to propose separate constructs of NJREs and doubts about actions, based on different apparent temporal scales and differences in their physical vs. cognitive nature. However, more work is needed to clarify the boundaries between these similar constructs. Distinctions between feelings of something not being just right and feared consequences could be incorporated explicitly into future questionnaire items. For example, respondents could be asked whether they perform an action (e.g., checking their alarm clock) because (a) I was afraid that if I didn’t check it something negative or bad would happen (e.g., my alarm clock wouldn’t go off and I would oversleep) or (b) I had an uncomfortable sensation in my body that something wasn’t just right. Finally, it will be important to further develop our conceptual model of NJREs. As we gather more information about NJREs, we can better articulate their relationship with obsessions and compulsions, what triggers may produce them, and what can be done to reduce the discomfort that they produce.
References available in original article on ScienceDirect.